https://www.fda.gov/food/outbreaks-foodborne-illness/investigations-foodborne-illness-outbreaks

 The U.S. Department of Agriculture’s Food Safety and Inspection Service (FSIS) is issuing a public health alert for ready-to-eat (RTE) salad products containing Food and Drug Administration (FDA) regulated peanut butter that has been recalled by J.M. Smucker Company due to potential Salmonella contamination. FSIS is issuing this public health alert to ensure that consumers
The U.S. Department of Agriculture’s Food Safety and Inspection Service (FSIS) is issuing a public health alert for ready-to-eat (RTE) salad products containing Food and Drug Administration (FDA) regulated peanut butter that has been recalled by J.M. Smucker Company due to potential Salmonella contamination. FSIS is issuing this public health alert to ensure that consumers
 Where the fresh organic strawberries were imported from was not disclosed.
Where the fresh organic strawberries were imported from was not disclosed.
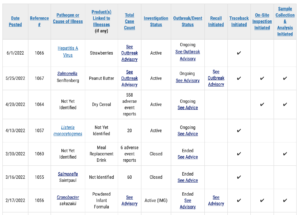
The Public Health Agency of Canada (PHAC) is collaborating with provincial public health partners, the Canadian Food Inspection Agency (CFIA) and Health Canada to investigate an outbreak of hepatitis A infections involving two provinces: Alberta and Saskatchewan.
Based on investigation findings to date, consumption
Thus far there are 16 reported cases of Salmonella Senftenberg in 12 states.
The product is being recalled from all states and Canada, Dominican Republic, Singapore, Malaysia, Taiwan, Korea, Thailand, Honduras, Spain, Japan.
Linked list of announced recalls – updated May 26, 2022
Primary Jif peanut butter recalls
Brookshire Grocery Company of Tyler, Texas has issued a voluntary recall of bulk Yellow Flesh Peaches available in stores between 4/15/22 and 5/17/22, because they have the potential to be contaminated with Listeria monocytogenes, an organism which can cause serious and sometimes fatal infections in young children, frail or elderly people, and others with weakened
The North Carolina Department of Health and Human Services is advising people to not eat or serve certain Jif brand peanut butter products that are being recalled due to potential Salmonella contamination.
On May 20, 2022, J. M. Smucker Company issued a voluntary recall of select Jif peanut butter products. Fourteen cases of Salmonella related
The J. M. Smucker Co. announced a voluntary recall of select Jif products sold in Canada due to potential salmonella contamination. If consumers have products matching the following description in their possession, they should dispose of it immediately. This information can be found on the product packaging. The product lot code range for the impacted
 Wayne Farms LLC of Decatur, AL, has expanded its nationwide recall of ready-to-eat chicken breast fillets because they may be undercooked, which can result in the growth of foodborne pathogens.
Wayne Farms LLC of Decatur, AL, has expanded its nationwide recall of ready-to-eat chicken breast fillets because they may be undercooked, which can result in the growth of foodborne pathogens.
The recall has been expanded from 30,285 pounds to 585,030 pounds. There are five new production codes — 23618, 24357, 24512, 24583, and 24957 —
 H-E-B is voluntarily issuing a recall for H-E-B Bakery Two Bite Brownies (12 oz) and H-E-B Simply Delicious Cookies with Brownie Bites Party Trays for potential metal fragments in product. The potentially affected products were manufactured by an outside supplier and distributed only to H-E-B and Joe V’s Smart Shop stores in Texas and Mexico.
H-E-B is voluntarily issuing a recall for H-E-B Bakery Two Bite Brownies (12 oz) and H-E-B Simply Delicious Cookies with Brownie Bites Party Trays for potential metal fragments in product. The potentially affected products were manufactured by an outside supplier and distributed only to H-E-B and Joe V’s Smart Shop stores in Texas and Mexico.